The Mandible Illusion
- Andre Chen

- Mar 7
- 4 min read
Updated: Apr 12
When Guided Surgery Meets Surgical Reality

“The map is not the territory.”
— Alfred Korzybski
March 8th, 2026.
The world woke up in a strange atmosphere.
Flights cancelled. Beirut atacked and just thinking that in 2 weeks I was supposed to be there for the straumann IEXCEL launch 🚀……..
The Middle East on fire.
Europe once again talking about war and nuclear weapons france 🇫🇷 doubling the nuclear warheads ….. a simple spark ⚡️ and war !!!
And while geopolitics shakes the planet, inside our clinics we continue our own daily battle — the battle against bone resorption, tooth loss, and anatomical limitations.
This week I had one of those moments that reminded me of my years at NYU, when we would spend endless hours discussing surgery, prosthetics and biomechanics as if implantology were a three-dimensional chess game played inside bone.
Because sometimes a case that appears simple…
ends up teaching us a great deal.
here we were me and Margarida on a a Friday afternoon…. Like the Jedi way a master and an apprentice …. This time we went for bilateral posterior mandible !!
Quadrant 4 — When Everything Works
Margarida started to perfora the case. Extraction of a molar and placement of two implants.
We used iGuide, and I must say it performed exactly as expected.
Drill by drill she made perfect implante placement !
The osteotomies were prepared precisely and two TLX 3.75 standard implants were placed.
No drama. 🎭 No deviations. No improvisation.
One of those rare surgeries where everything follows the plan perfectly. I even though and stated “this iguide works better in Margaridas hands than in mine “….
Implants placed right on the spot. Chapeau.
we move for Quadrant 3 — “ The Mandible Shows Its Teeth”
Then we moved to the third quadrant. And the situation changed completely.
We were dealing with:
moderate horizontal atrophy
significant vertical resorption
a pronounced lingual concavity
On the CBCT it looked like we had 20 mm of bone. In reality? Probably 8 or 9 usable millimetres.
This is what I like to call the posterior mandible illusion. The lingual concavity creates a false sense of security. You look at the scan and think:
“We have plenty of bone.”
But once the flap is opened…
the anatomy tells a different story.
The Classic Posterior Mandible Mistake
There is another frequent mistake in this region.
Trying to place implants perfectly vertical.
But the posterior mandible is rarely vertical.
If we remember the classic removable prosthodontic literature, we know the mandible undergoes centrifugal resorption over time.
This alters the relationship between the cortical plates. Implants often need to follow the natural occlusal curvatures:
the Curve of Spee
the Curve of Wilson
Which means that a slight lingual inclination is frequently the correct prosthetic orientation.
Otherwise something very common happens.
The implant is placed vertically…
and the prosthetic access emerges too buccally.
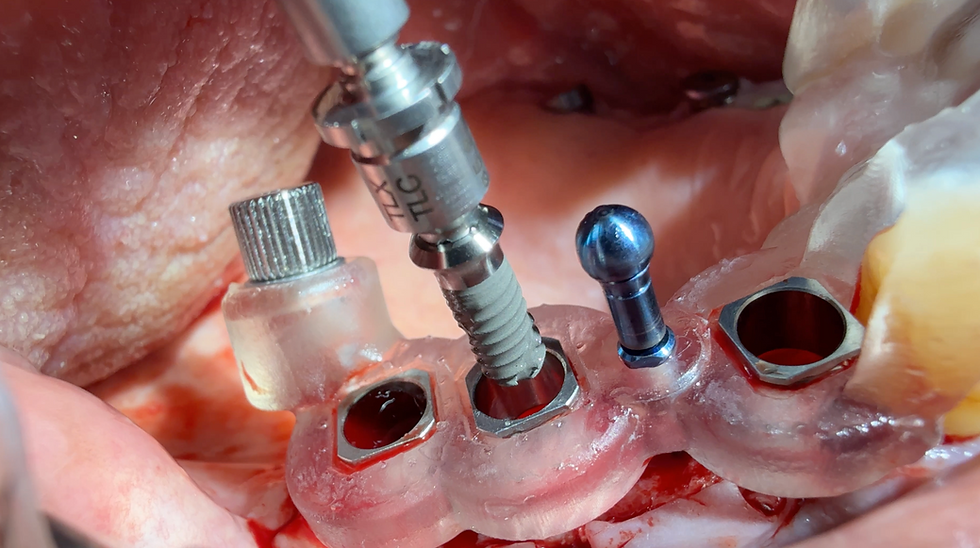
When the Drill Decides Its Own Path
During the osteotomy preparation we encountered one of the classical limitations of guided surgery.
The drill enters perfectly through the guide.
But once it contacts the bone… it slips … it doesn’t really engage the osteotomy !
This tends to happen when we have:
thin ridges
dense cortical bone
irregular ridge morphology
That is exactly what happened in the 36 site.
The osteotomy deviated slightly toward the buccal side.
And when the implant was inserted… it became clear that it was too buccal.
The Moment of Surgical Judgment
at this point the Brazilian embassador in Portugal just come in the clinic with an emergency 🆘 a wisdom tooth hurting !! And of course I broke two roots and took me 40 minutes to remove it !!
While in margaridas surgery …….This is where implant dentistry becomes real surgery.
You can either follow the guide blindly Or adapt to the biology in front of you.
We decided to remove the misplaced implant.
The osteotomy was slightly deepened.
Space was created with a high speed bur on the crest to position the platform crestally, reducing exposure of the rough implant surface.
Small adjustments. But with major three-dimensional consequences.
The Critical Area — Site 34
At the 34 site the situation was even more extreme.The resorption had progressed to the point where the buccal and lingual cortical were almost fused.
The ridge was extremely thin. And before the surgery we anticipated this moment …
The strategy here was to gain apical anchorage in trabecular bone, accepting that part of the implant would inevitably remain exposed on the buccal aspect.
In this region implantology stops being cosmetic. And becomes pure biomechanics.
A Detail That Rarely Appears in Digital Planning
Another interesting difficulty appeared during drilling. The mandibular canine. Large root. Significant volume.
And suddenly the contra-angle begins to hit the tooth. The drill loses angulation.
The osteotomy becomes technically challenging.
These are the small realities that rarely appear in digital planning software.
But they appear every day in real surgery.
BLX… or Maybe Not
We also discussed which implant macrogeometry would be ideal in this scenario.
A BLX implant, with its aggressive threads, can sometimes create challenges in very thin bone.
The implant may:
engage too early
deviate during insertion
lose the prosthetic axis
Perhaps a slightly more passive macrogeometry would have been easier to control.
Nevertheless, with careful manual control we managed to position the implant correctly in three dimensions.
The Human Factor
At the end of the procedure another factor appeared.
One that is rarely discussed in lectures.
Patient fatigue.
The patient was already quite tired. We therefore performed a moderate regenerative procedure:
particulate biomaterial
resorbable membrane
modest volume reconstruction
With more time and patient comfort, the regenerative phase could probably have been more elaborate.
The Real Lesson
Modern implant dentistry has extraordinary tools.
Digital planning.
Guided surgery.
Dynamic navigation.
But no technology replaces three fundamental principles:
Anatomical knowledge.
Proper osteotomy preparation.
Intraoperative decision-making.
The guide may show where we want to go.
But only the surgeon can decide how to get there.
Clinical Pearl
1 - The posterior mandible may appear to have abundant bone on CBCT imaging. However, the lingual concavity frequently reduces the real available bone volume.
2- Digital planning is essential. But anatomical reading and surgical adaptability remain irreplaceable.
“In implant dentistry the guide shows the plan.
The surgeon understands the bone.”
But even with all this rollercoaster 🎢 surgery with embassadors in the middle the performance was good margarida did a wonderfull job and Mr Abrantes will have a nice rehabilitation done ✅!!
Have a nice weekend!!
Andre
Comments